Charlie Peck knew that as his voice transitioned from female to male during hormone replacement therapy, his old, higher-pitched voice would be gone. In the hopes of creating a work that at once recorded his transition and growth while paying tribute to the transgender community, he recorded his a song using his voice prior to HRT. Nine months later into the therapy for his transition, he recorded a second vocal track using his new, deeper voice.
Speaking to The Huffington Post, Peck explained his pursuit of the unique project. He saw his voice as a filter through which so many of one’s thoughts travel, and documenting its change during therapy would serve as a record of his journey, stating, “In contact with other humans, the filter through which everything you say is perceived is your voice. I was also really scared that I would not be able to sing any more. With these thoughts in my head an idea about singing as a way to show others my journey started to form. When I contacted my very talented friend, André Åhl Persson, who is also a musician, and he was willing and thrilled to do this project with me this seed of an idea started to grow.”
Though the track has been garnering attention from the public at large, serving as a boon to his music career, he’s insistent that this was done for personal and ideological, rather than professional reasons. He continued, “You are not alone, things can get better and put yourself before everybody else’s expectations on how you should live your life. Now that I have the energy to give something back to the trans* community―this is my heart medicine for those in need.”
Photo credit: Spencer Platt/Getty Images – Many U.S. apartments have individual heating and cooling systems that are less efficient than current technology.
People who rent their homes, or don’t have enough money to make major upgrades to their homes, have for many years been left out of a major shift in heating and cooling technology that can improve efficiency, save money and be better for the global climate: heat pumps.
Heating and cooling buildings consumes 35% of all the energy used in the United States each year. Many homes and businesses are converting their fossil fuel-powered heating and cooling systems to electric-powered heat pumps, which use electricity not to generate hot or cold air but to move heat into spaces needing warmth and out of spaces needing cooling.
Until recently, that process has required a significant amount of sizable and expensive equipment to be permanently installed in a building, which needs a professional contractor and can cost as much as US$10,000 just for the installation – in addition to the actual equipment. Often called mini-splits, these systems usually have a condenser outside the building that exchanges heat with the outdoor air and an evaporator inside that exchanges heat with the indoor air.
The New York City Housing Authority has been installing window-mounted heat pumps in apartments, like this one in Queens. AP Photo
But now window heat pumps are becoming available in the U.S. Much like a window air conditioner, these self-contained devices can be installed without professional help and plugged into a wall outlet. Unlike window air conditioners, though, they can provide heat as well as cooling. They cost much less than a permanent system – between $3,000and $4,000 – and can be moved to a new property if the owner relocates.
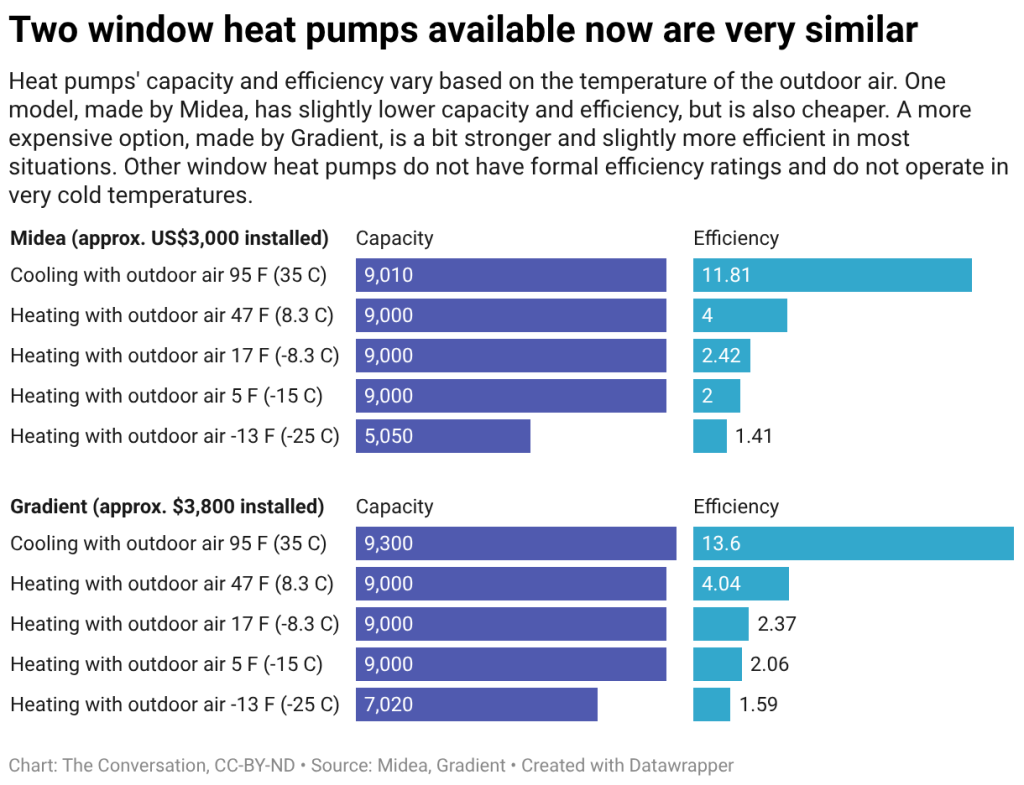
There aren’t many options commercially available yet, and those on the market can’t heat or cool very large spaces on their own. And they work less efficiently when heating homes in places with extremely cold outdoor temperatures. A few models are available on the market that are even cheaper, but they don’t have efficiency ratings, don’t work when outdoor temperatures are very cold, and are louder when running.
Heat pumps use a reversible refrigeration cycle and can provide similar heating and cooling as electric-powered space heaters, furnaces and baseboard heaters, while using less than half the electricity.
The most common heat pumps transfer heat between air indoors and outdoors, but other systems can exchange heat with the ground or with bodies of water, such as lakes.
Heat pumps’ capacities are defined by the amount of heat they can transfer in a particular period of time. A heat pump serving an entire home may need a capacity of 12,000 to 60,000 British thermal units (about 12,660 to 63,300 kilojoules) – but the window units’ capacities are much lower, getting up to only about 9,000 Btu (9,500 kJ).
Performance varies based on the conditions outdoors, where the unit is either sending excess heat to cool the indoors or gathering heat to warm the indoors. In cooling mode, heat pumps are rated by their seasonal energy efficiency ratio, a figure that indicates how much cooling is achieved per unit of electricity used. The corresponding measurement for heating is called heating seasonal performance factor. In general, the larger these numbers are, the better they will perform. The U.S. Department of Energy has established minimum standards for those figures.
While these units operate even when outdoor temperatures are -13 degrees Fahrenheit (-25 degrees Celsius), their heating output is reduced to almost half of its rated capacity, and their energy efficiency falls to one-third of its rated performance at that temperature.
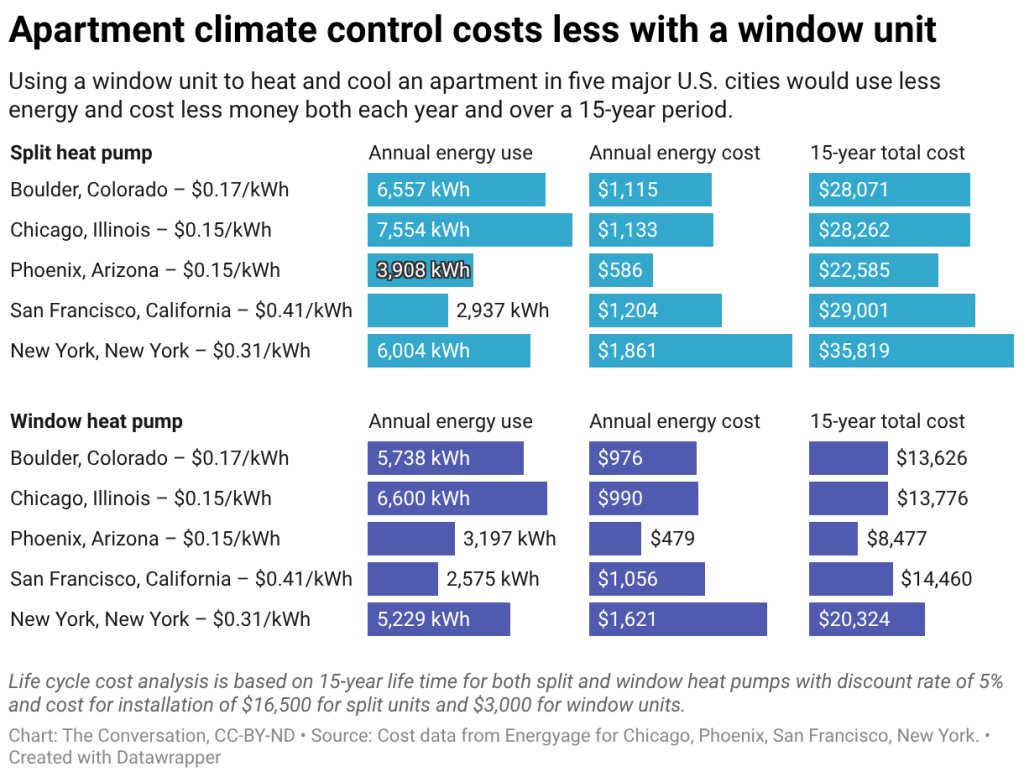
In addition to their low cost compared to conventional split heat pumps, packaged window heat pumps meet heating and cooling needs with lower energy demands and costs. But each window unit serves just one room, while a more common split unit can serve multiple rooms.
Packaged window heat pumps are easy and inexpensive to install and offer all-in-one heating and cooling options for apartments and older homes, with higher energy efficiency performance than traditional systems. Their main limitations include their low capacities and reduced energy efficiency in extremely cold climates or conditions.
Photo credit: AP Photo/John Locher – A recent settlement with farm equipment manufacturer John Deere made it easier for farmers to repair machines on their own, a win for the ‘right to repair’ movement.
The “right to repair” movement is gaining steam as consumers push corporations to offer them more freedom to fix products – from cars to dishwashers to toys.
In April 2026, farm equipment maker Deere & Co. inked a US$99 million settlement in a class action suit over its prohibition on independent repairs to its increasingly high-tech equipment – another win for the movement. While the company didn’t admit wrongdoing, it will let farmers make more repairs themselves.
Equally significant, this case showed that the Federal Trade Commission, a lead plaintiff, may be more willing to protect consumers against the growing corporate control over servicing products after purchase.
Even President Donald Trump has weighed in. At an Oval Office event on June 4, 2026, he described existing restrictions as “strange” after he met with auto executives. “Nobody’s allowed to fix their car. … So I thought we’d do something about that,” he said, without offering details.
This push is understandable. As consumers want more reliable products, gaining the right to repair them with their own parts makes sense.
But they often overlook existing protections in their product warranties, which obligate the manufacturer to repair or replace if something goes wrong.
As a scholar focused on operational sustainability in supply chains, I have found that strong warranties aren’t just a safety net for buyers. They help companies build trust and stand out. Hyundai and Apple, for example, have used strong warranty programs to keep customers coming back for repairs within their own networks while maintaining profit margins. But many shoppers overlook this tool as the political momentum for the right to repair grows.
Back to the 1970s
Many automotive and electronics manufacturers have been making it harder for consumers to use parts not produced or authorized by the original manufacturer. For example, data can be transmitted back to the manufacturer in real time and flag a part from an independent supplier as incompatible.
Another common tactic is the use of “warranty void” stickers, which claim that repairs done by a third-party service will cancel the manufacturer’s product warranty. These practices have drawn widespread criticism for suppressing competition and encouraging planned obsolescence – and are among the main targets of right to repair advocates.
But consumers have a tool that’s widely underused: A 1975 law that prohibits voiding a warranty simply because an independent mechanic or a part from an independent vendor was used. This measure was designed to discourage the production or sale of low-quality products and sought to protect consumers from excessively restrictive coverage and bad-faith corporate negligence.
It was this law as well as several other consumer protections that the Biden administration’s FTC cited in 2024 when it warned several companies that they improperly restricted their warranty terms.
One reason consumers are largely unaware is that most find the text of warranty terms and the disclaimers difficult to read. And this isn’t an accident. Many manufacturers see warranties as sunk costs that should be avoided, and they have no incentives to clarify the terms or honor them.
Trust pays
Companies should rethink their approach to warranties – because it makes good business sense.
When manufacturers see they can no longer prevent third-party repairs, or offer warranties that are hard to redeem, it’s usually because they decide it’s more cost efficient to produce low-quality products. But that choice often cuts into the producer’s own profit while leaving the consumer worse off – and has a worse environmental impact, a recent study suggests.
Hyundai vehicles, including the Kona electric car, have built up customer loyalty through the flexible warranties offered by the automaker. AP Photo/Martin Meissner
A smarter option for manufacturers would be to establish a better, more efficient service network and offer more attractive warranty programs to retain customer loyalty.
Some companies have demonstrated that strong warranties pay off. Outdoor apparel maker Patagonia offers an “ironclad guarantee” to repair or replace its products for any reason. The “all mighty guarantee” offered by Osprey, which also manufactures outdoor gear, will repair or replace any damaged or defective product free of charge.
Then there’s retail giant Costco’s automatic extension of manufacturers’ warranties on major appliances and electronics – a major driver of its success.
Meanwhile, under the right to repair measures currently proposed, the post-purchase service and repair markets would likely get more competitive. New rules would let outside service providers and warranty companies gain better access to fix the products. Extended warranties and service contracts would then become even more prevalent, and manufacturers would need to become more vigilant.
Consumers also need more protection from the FTC, the top federal regulator tasked with consumer protection. Indeed, the right to repair movement reflects, in part, public disappointment that the government has failed to serve as a watchdog amid misleading corporate claims about warranty protections.
While the FTC has occasionally sued companies to protect consumer rights under the 1975 law, it has the legal tools to be more aggressive. Such a shift would not only change the corporate culture around warranties but send a message to consumers that warranties should work for them.
Enforcement, not just choice
If manufacturers embraced stronger warranty enforcement, consumers would benefit the most, provided they’re aware of what these protections entail. But manufacturers would come out ahead, too. By building up efficient service networks and offering more versatile warranties, they would remain competitive and foster customer loyalty, Hyundai being a good example.
The right to repair movement is in many ways a live policy experiment on expanding access to repair markets and giving consumers more choices. But more choices don’t necessarily lead to a better outcome. Coupling repair rights with stronger warranties and better enforcement is the best way a company can claim the prize it always says it wants: more satisfied consumers.
According to some estimates, the average time dads spend caring for their kids each day has quadrupled over the past 50 years. Their attitudes about parenting are also changing. Today, men are about as likely as mothers to say parenting is a key source of meaning and a central priority in their lives. Roughly 85% of fathers identify parenthood as one of the most important aspects of their identity.
But there’s a less encouraging trend tucked into these gains. More is being asked of dads – and moms, for that matter – because the extended family and community networks that once supported childrearing have shrunk or deteriorated.
One society he studies, the Aka Pygmies of the Central Congo, have been called “the best fathers in the world” for their dedication to childcare. Aka men are frequently observed within arms reach of their infants and take a lead role in raising them. Children are seen as central to men’s lives.
However, if you compare the time Aka dads spent on childcare with recent data on American parents, as parenting writer Tomo Kumaki recently did, you might be surprised.
According to 2024 American Time Use Survey data – considered the gold standard of evidence on how Americans are spending their time – American dads of infants are devoting about 125 minutes a day to what’s called “primary child care,” in which their main activity is tending to the child. They’re spending another 394 minutes on what’s known as “secondary child care,” which involves watching a child while doing something else, such as cooking dinner or straightening up the house.
The minutes American dads relayed should be taken with a grain of salt; it’s a stretch to compare an anthropologist’s direct observations with self-reported time diary data, which can often be subject to bias. Still, it’s striking to see how – based on these calculations, at least – today’s new dads are devoting far more time to parenting than a society described as having the best dads in the world.
Among the Aka people, who are indigenous, nomadic hunter-gatherers native to Central Africa, men take a lead role in raising their children. Andia/Universal Images Group via Getty Images
When I spoke with him about how fatherhood has changed, Hewlett told me he thinks the role of fathers has taken on more importance today than ever before – not just because mothers are more likely to have jobs outside the home, but because there are simply fewer childcare helpers around.
When you’re surrounded by your kin and neighbors in a communal setting like the Aka, it’s easy to get assistance with kids. Fathers care for children, but so do lots of other people.
A 2021 study of another hunter-gatherer society, the Agta, which lives in the mountains of the Philippines, found that fathers provided only about 7% of child care. Mothers, however, provided only about 25%. The rest came from siblings, grandparents, extended family, peers and other community members, who all pitch in.
A class divide
In much of the industrialized world, daily life is organized around the nuclear family, with relatives and neighbors playing a less central role than they once did.
Today’s fathers contribute more to childcare than even the most hands-on hunter-gatherer dad, because there’s simply less of a village to support shared care.
Even as men are being asked to take on a bigger role in childcare, it’s become harder for some men to do so. That’s because – in the U.S., at least – the time men are able to spend on childcare has become increasingly stratified by class.
Journalists Derek Thompson and Aziz Sunderji analyzed multiple waves of U.S. data collected by the Multinational Time Use Study and were able to show that the significant rise in the time dads spend parenting over the past 60 years has primarily been driven by college-educated fathers.
When the Multinational Time Use Study started in the 1960s, fathers with a college degree were devoting only a few extra minutes per day to childcare compared with noncollege-educated dads. But the gap has quintupled over that time span, such that college-educated dads are now spending 46 more minutes with their kids each day compared with noncollege-educated dads.
So why the growing divide? In part, it’s because benefits such as universal paid paternity leave and stable, flexible work options are available only to dads with good jobs.
Only about half of U.S. fathers take any paid paternity leave following the birth of a new baby, because many employers don’t offer it. In theory, most dads who can’t access paid leave should be eligible for unpaid leave through the 1993 Family and Medical Leave Act. However, since that legislation doesn’t apply to small businesses or many part-time or gig work situations, about 44% of workers are ineligible for it. Low-wage dads are also often reluctant to take leave because they can’t afford to lose income.
The rise of what sociologists call intensive parenting among the most educated, affluent parents also helps account for some of the class divide in parenting time. As the wealth gap between the richest and poorest Americans has widened over the past 60 years, many parents have been eager to optimize their children’s success. Devoting extra time to children, including monitoring their schoolwork and enrolling them in enrichment activities that require time and money, has become one way for parents with privilege to give their children a leg up.
In my view, hands-on parenting should not be a luxury good. Americans should be fighting for policies that empower all dads, no matter their income, to enjoy time with their children. The village could use some rehabilitation, too, since parents fare best when they have access to community support and stronger connections with their neighbors, friends and family.